
{kind=link}
Complementary and alternative medicines (CAM) are medical products and services that are considered “outside” conventional medicine, but are intended to prevent or treat illness. CAM is big business, and widely used: Most Americans take some sort of supplement. While CAM is purported to be effective for many medical conditions, the evidence supporting routine use is very limited. Heart failure is a common cardiovascular disease affecting over 6 million Americans and causing substantial morbidity and mortality. A scientific statement from the American Heart Association was recently published and is intended to give patients, the public, and health professionals a comprehensive summary of the efficacy and safety of CAM in patients with heart failure.
What is heart failure
Heart failure, also called congestive heart failure, is a chronic, progressive medical condition that is the result of your heart’s inability to meet the needs of the body. In heart failure, a weak heart cannot supply the body with enough blood. It can occur when the heart cannot fill with enough blood and/or when the heart is too weak to pump properly. Symptoms include weakness and difficulty with activities like walking or climbing stairs. Heart failure can cause the heart itself to adapt (enlarging and developing more muscle mass) and also cause a number of compensations in the body that may partially alleviate some of the problems, while causing other problems (e.g., kidney and liver damage). There are two main types of heart failure (left sided vs right sided, referring to the sides of the heart) that can affect the treatment approaches taken.
Treatments for heart failure are determine based on the type of heart failure and the underlying cause. Core recommendations include regular exercise, ceasing any tobacco use, and managing conditions like hypertension and high cholesterol. Surgery or other interventions may be appropriate (e.g., coronary artery blockage) and medications may be recommended depending on the severity of the disease. The overarching goal is to control symptoms and preserve/extend quality of life.
CAM for heart failure
As has been pointed out in many prior posts, CAM is not regulated like conventional medicine in most countries. Regulators tend to use a “light touch” with these products and generally do not subject them to the same requirements for manufacturing or for evidence to support any claims of efficacy. It is perhaps because of this confusion that CAM is widely used despite a general lack of evidence to suggest these products are high quality, safe and effective. It is estimated that over 30% of heart failure patients may be using CAM.
Given the popularity of CAM and the importance of medical therapy for the treatment of heart failure, patients and practitioners alike need to understand the effects, benefits and risks of CAM in the management of this disease. To support this, a group of cardiologists, pharmacists, scientists and a nurse practitioner undertook a comprehensive literature search to identify (1) evidence for efficacy of CAM in heart failure and (2) evidence on the safety of CAM, including the repercussions of combining CAM with heart failure medications.
The paper is titled “Complementary and Alternative Medicines in the Management of Heart Failure: A Scientific Statement From the American Heart Association” and it was published in December, 2022. The statement includes a detailed summary on the oversight and regulation of CAM (from a US perspective) but also discussed global utilization trends. The authors caution that health care professionals and patients should be aware of the regulatory status of CAM if considering these therapies.
CAM efficacy in heart failure
Several CAM products have been investigated in clinical trials, and some have been associated with improvements in symptoms, functional capacity and quality of life. The report has a detailed summary of the mechanism of action (if known), the evidence, known benefits, and harms. I’ll provide a short summary and highlight some of the products here, but please refer to the report for the full details.
Alcohol – I wouldn’t consider alcohol CAM, but this statement does. Observational data suggests low-to-moderate amounts of alcohol may be associated with a reduced risk of developing heart failure. Habitual consumption or abuse of alcohol is a known cause of cardiomyopathy (heart enlargement) and heart failure.
Coenzyme Q10/Ubiquinone/Ubiquinol – CoQ10 occurs naturally in some foods and is a cofactor in many biologic pathways. Administration of large amounts has been shown to have modest effects on ventricular function and quality of life in small trials. The largest randomized trial (I blogged about it back in 2013) had no effect on some measures but did reduce major cardiovascular events at two years. Given the overall quality of the evidence the report says CoQ10 has “uncertain value”.
Omega-3 Polyunsaturated Fatty Acids/Fish Oil/Eicosapentaenoic Acid/Docosahexaenoic Acid – Omega-3 polyunsaturated fatty acids (PUFAs) are found in foods like fish, soybeans and organ meats. These supplements have been extensively studied, and while not a slam dunk, there have been benefits shown that include reductions in hospitalization and improvements in ventricular function. Some cardiovascular guidelines recommend PUFA consumption. The report is supportive of supplementation (but not at the expense of guideline-directed medications) at doses of <4g per day.
Thiamine/Vitamin B1 – Thiamine is a water-soluble vitamin found in grains, legumes and yeast. Severe deficiency is a documented cause of heart failure. Many heart failure patients have a relative deficiency from chronic diuretic (water pill) use, dietary factors and age. However, supplementation does not appear to be worthwhile (and is not recommended) unless there is a clinically significant thiamine deficiency present.
Vitamin D/Ergocalciferol (Vitamin D2)/Calcifediol (23-hydroxyvitamin D)/Cholecalciferol (Vitamin D3)/Calcitriol (1,25-Dihydroxycholecalciferol) – Vitamin D naturally occurs in food and has been touted as a panacea for just about everything. Supplementation has shown to have positive effects on some markers, but not others. The VITAL_HF trial examined 2,000 IU of vitamin D per day over 5 years and did not reduce the risk of a first heart failure event compared with placebo. The overall evidence is felt to be inconclusive.
Yoga and Tai Chi – Both yoga and tai chi are felt to be safe, effective, and well tolerated therapies for heart failure. Small trials show improvements in walking distance and lower depression scores as well as improvements in quality of life. While the evidence is overall modest, the report describes them as having “promise” as beneficial forms of exercise.
CAM harms in heart failure
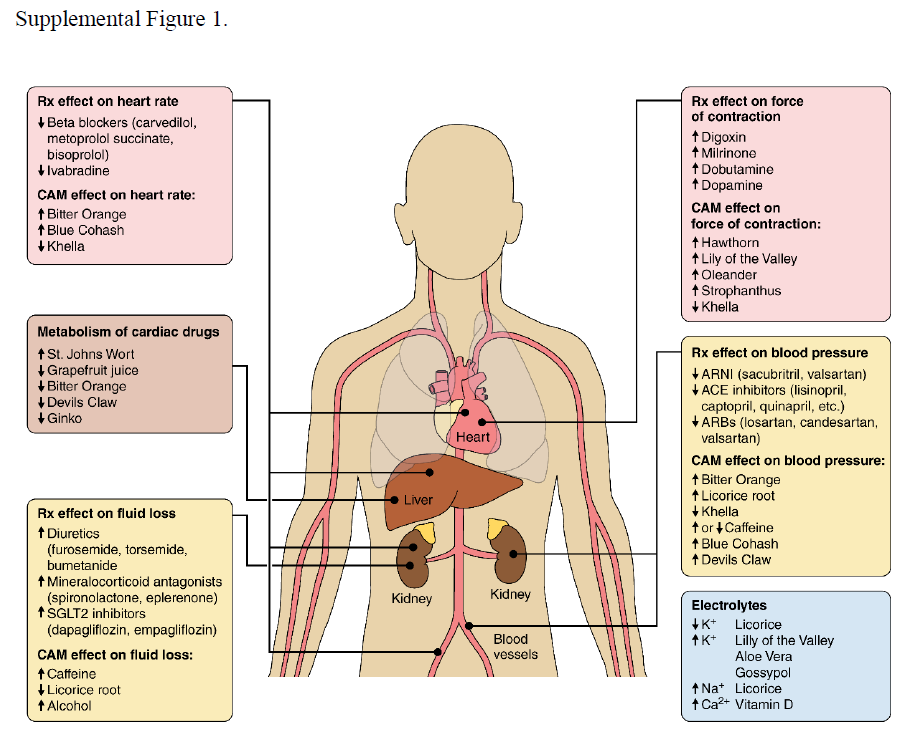
There is an extensive list of supplements that may cause drug interactions:

CAM can have negative effects through different mechanisms:
Alcohol – Excessive alcohol, as noted above, has harmful effects. Consumption of >10 drinks per week is associated harmful effects.
Caffeine – The effects of caffeine on heart failure seem neutral to possibly negative. Avoidance of excessive amounts seems to be warranted, and caffeine may present a greater risk in those sensitive to its effects.
Gossypol – This is a compound derived from the stem, seeds, and roots of the cotton plant, and has been used as a male contraceptive and also an antimalarial. Consumption depletes potassium (bad if you have heart failure) and chronic use can cause circulatory problems.
Grapefruit Juice – I’ve blogged about how grapefruit juice can cause drug interactions in a past post. Given grapefruit juice can affect the absorption of several drugs used to treat heart failure, the report recommends complete avoidance given the unpredictable effects.
Hawthorn – Seems to have some positive effects on heart contractility but may interact with a common heart failure drug, digoxin.
L-arginine – While l-arginine is an amino acid that occurs naturally in food, RCT data of supplements shows an increase risk of death and is not recommended.
Licorice – Glycyrrhetinic acid is an active metabolite of black licorice and has negative effects on heart failure. While I am not certain how much of this is found in candy products like Twizzlers, the report notes that red licorice has no associated risks.
Lily of the Valley, Oleander, Strophanthus, Ouabain – Digoxin, identified from the digitalis plant, is commonly used to treat heart failure. However, many other plants, like lily of the valley, have been identified to contain related chemicals. Because of the narrow range between beneficial and toxic doses, self-medicating with natural plants is a dangerous and potentially fatal alternative to using digoxin medically.
Vitamin E – Supplement doses in excess of 400 IU/day may increase the risk of heart failure and so use with caution is advised.
Conclusion: Limited benefit for CAM
CAM is undoubtedly popular and may be used alongside conventional treatments for heart failure, or in place of evidence-based therapies. While there are a few products (e.g., PUFAs) and approaches (e.g., yoga/tai chi) that may be beneficial, there are also a large number of products that can worsen heart failure or cause negative interactions with prescribed medications. While additional research is undoubtedly advisable, taking a cautious approach to CAM use (of any kind) would seem to be the safest strategy with the lowest risk of unanticipated harm.